
 1")
Table of Contents Show
Postpartum hemorrhage is defined as heavy uncontrolled vaginal bleeding after childbirth. Losing lots of blood may cause a severe drop in your blood pressure. If not treated properly, it further results in shock and eventually death.
Normally, postpartum bleeding will last for two to three weeks after delivery. It should be like a period or less and gradually resolve over time, but if it continues with heavy bleeding for weeks, it may be a postpartum hemorrhage.
About 5 in 100 women have postpartum hemorrhage (PPH). In cesarean birth delivery, there is a high risk of PPH. It happens after the placenta is delivered but can also happen later. Causes of postpartum bleeding may include a bleeding disorder or placenta tearing.
A C-section is surgery in which your baby is born through a cut that your doctor makes in the uterus. After delivery, it’s quite normal if you are losing some blood.
Women usually lose about 500 milliliters during vaginal delivery and about 1,000 milliliters after a C-section or cesarean birth.
But if you are losing much more blood, which is what makes it a dangerous condition and leads to postpartum hemorrhage. PPH occurs after delivery or up to 12 weeks.
Types of postpartum hemorrhage
There are mainly two types of PPH:
- Primary postpartum hemorrhage (which occurs within the first 24 hours after delivery)
- Secondary postpartum hemorrhage (which occurs 24 hours to 12 weeks postpartum)
Stages of postpartum hemorrhage
 3")
After delivery mother goes through three postpartum bleeding stages: lochia rubra, lochia serosa and lochia alba.
Stage 1: Lochia Rubra
The first stage of postpartum bleeding is Rubra, lasting up to four days postpartum. It will be dark or bright red and very heavy sometimes. In lochia, it is very typical to see the clots.
Stage 2: Lochia Serosa
The second stage of postpartum bleeding is serosa, lasting about two weeks after delivery. Its colour will change from light red to a watery pink or pinkish brown.
You can still see blood clots during this stage, though clots should be smaller in comparison to the lochia rubra.
Stage 3: Lochia Alba
Alba is the third stage of postpartum bleeding that can last for two to six weeks after delivery. Lochia changes from pink to a light brown to a yellowish-white colour.
The main cause of postpartum hemorrhage
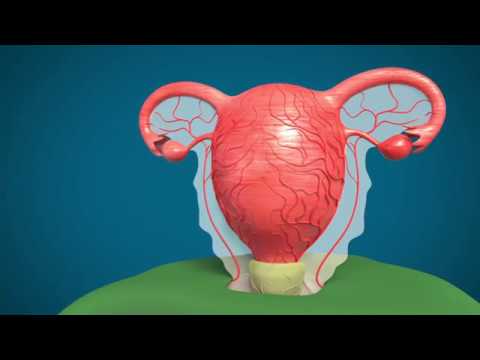
Once a baby is delivered, uterine contractions push back the placenta. After the placenta1 is delivered, these uterine contractions help to put pressure on the bleeding vessels in the placenta attachment area. If the uterus does not contract enough after delivery, it may result in postpartum hemorrhage.
If the uterus does not contract strongly enough, these blood vessels bleed freely, and PPH occurs. If small pieces of the placenta stay attached, excessive bleeding is also likely.
These contractions aren’t strong enough to stop the bleeding (uterine atony). It is the main cause of PPH in 80% of cases.
PPH occurs due to:
- tear in a blood vessel in the uterus or vagina tear
- Uterine atony (or uterine tone) is when your uterine muscles don’t contract enough to stop the placental blood vessels and leads to uncontrolled bleeding after delivery.
- bleeding into a hidden tissue in the pelvis
- Blood clotting disorders or disturbances in clotting factors(thrombin)
- Placenta damage or uterine rupture
- Retained placental tissue, when the placenta doesn’t separate from the uterine wall.
Risk for postpartum hemorrhage
Approximately 40% of hemorrhages occur in women without any risk factors. Women are at greater risk for postpartum hemorrhage because of some factors. Risks for postpartum hemorrhage include:
- Prolonged labour
- fetal macrosomia (over 4000 g)
- Infection and Obesity
- Placenta got detached from the uterus too early during delivery
- Placenta previa
- If the uterus is larger than usual because of too much amniotic fluid or a large baby, known as an over-distended uterus
-
Use of forceps or vacuum-assisted delivery
-
Being of Asian or Hispanic ethnic background
- Multiple-baby pregnancy
- Placental problems like placenta previa and retained placenta
- Having twins, triplets, or more.
- Give birth to a large baby (<9 pounds)
- Too much amniotic fluid.
- Preterm labor or prior cesarean scar
- Tocolytics to stop labour
Symptoms of postpartum hemorrhage
The most common symptom of postpartum hemorrhage is continuously excessive bleeding after delivery. Postpartum hemorrhage includes other common symptoms:
- Uncontrolled blood loss
- Blood clots bigger than a plum
- Bleeding that soaks more than one sanitary pad an hour and doesn’t slow down or stop.
- Dark red bleeding even after the third day of delivery
- Drop-in pulse and blood pressure
- Increased heart rate and pale skin
- Decrease red blood cell count
- Worsen pelvic or abdominal pain
It would help if you had to be honest with your healthcare providers about how you’re feeling after delivery. Most PPH occurs without any common symptoms.
You must contact your healthcare provider immediately if you feel any of the symptoms of postpartum hemorrhage above in the days or weeks after delivery.
How is postpartum hemorrhage diagnosed?
Your healthcare provider will ask for complete medical history and health history, then a physical exam. They may also detect PPH based on the amount of blood loss and blood flow.
Measuring the volume of collected blood and weighing the blood-soaked pads after delivery is one common way to diagnose how much blood is lost.
Doctors recommend some tests to diagnose postpartum hemorrhages.
- Detection by estimation of how much blood you have lost
- Testing by blood tests for red blood cell count
- Continue monitoring on blood pressure and uterus bleeding
- Ultrasound to the image of your uterine blood vessel and other organs.
How is postpartum hemorrhage treated?
Treatment depends on what’s causing your bleeding vessels. Treatment aims to stop bleeding blood vessels, which may include:
- uterine massage to stimulate uterus contractions
- Repair cervical, vaginal, and uterine lacerations.
- In the uterus, by removing the remaining pieces of the placenta
- Packing uterus with a sterile material for sealing bleeding blood vessels.
- Use a catheter to put pressure on your uterine walls.
- Uterine artery embolization to repair the uterine rupture
- Blood transfusion with medication
- Having surgery: Laparotomy is done to open the lower abdomen to detect postpartum hemorrhages and seal bleeding blood vessels.
- Hysterectomy. This is surgery to remove the uterus and other pelvic tissues.
- Physical massage: Your provider can massage the uterus to help it contract, lessen bleeding and help the body pass blood clots. Your doctor may also give you some medications like oxytocin that help lessen bleeding and uterine contraction.
Replacing lost blood is important in treating postpartum hemorrhage. The doctor will give you a quick shot of IV 2(intravenous) fluids, products to prevent shock, and blood. Oxygen may also be given to treat it, and medications help induce contractions if uterine atony has caused bleeding blood vessels.
The most common drugs used are methylergonovine, oxytocin, or prostaglandins like misoprostol and carboprost.
In rare cases where medications don’t work, hysterectomy or laparotomy is the last option to stop the excessive blood loss.
Prevention of PPH
The best way to prevent postpartum hemorrhage is to identify it before delivery if there is a high risk. It is dependent on your complete medical history and symptoms. Routinely giving medications like oxytocin at the time of delivery helps to stimulate uterine contractions.
It is important to increase iron intake and red blood cell levels during pregnancy, decreasing the chances of PPH occurrence.
An excessive amount of blood loss can cause a severe drop in blood pressure,3 increased heart rate, and rapid breathing that can affect the blood flow to your liver, brain, heart, or kidneys and disturb the formation of blood products.
Do not use tampons. Regular menstrual pads just don’t cut it. It may also be possible that you may use many pads in one hour. Using tampons after delivery may lead to danger to the uterus and reproductive health.
Conclusion
Postpartum hemorrhage is a potentially severe and fatal condition. Mothers can lose large amounts of blood in a short period and causing a sharp decline in the mother’s blood pressure.
Postpartum hemorrhage is a medical emergency and needs to be treated right away. To prevent this fatal disease, accurately assess the risk factors and blood loss during delivery.
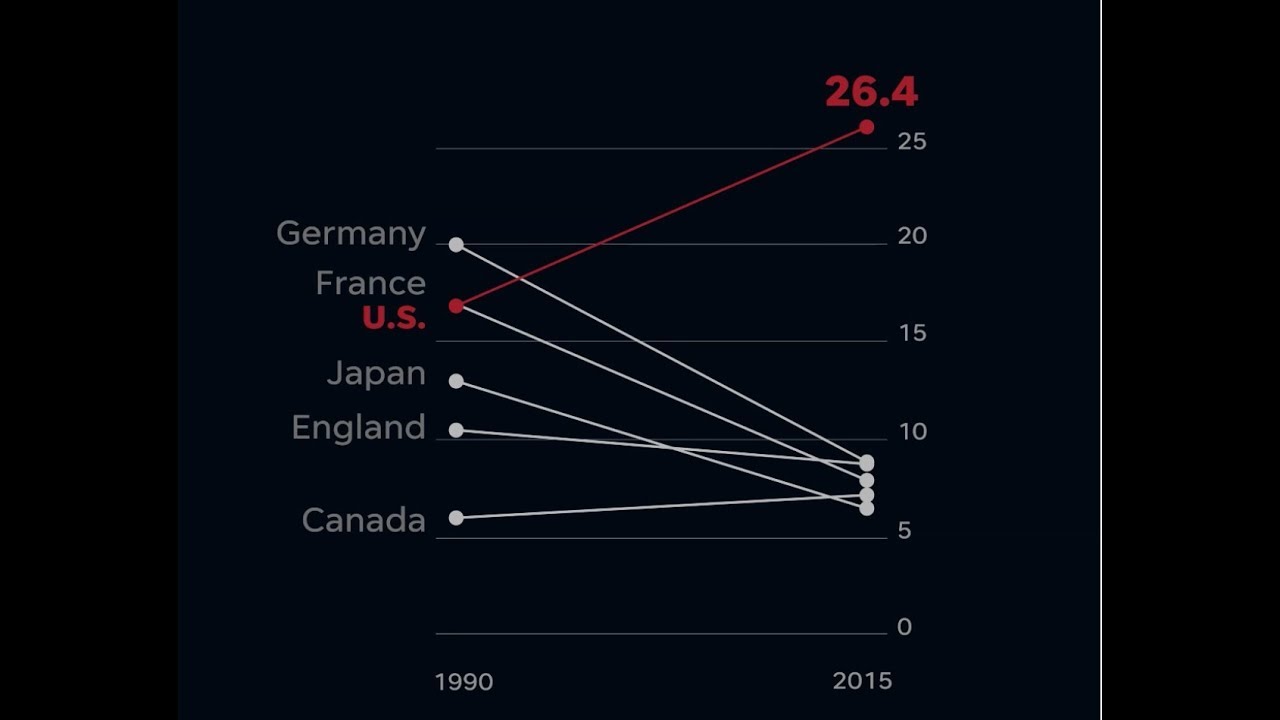
Hemorrhage is a major contributing factor to maternal morbidity and mortality. Although current data do not support any one method of quantifying blood loss as superior to another, quantifying blood loss, such as using graduated drapes or weighing, provides an accurate assessment of blood loss.
Postpartum hemorrhage occurs in about 1% to 10% of pregnancies. Postpartum 4hemorrhage may occur at delivery or soon after. You may experience heavy bleeding even after you go home from the hospital after delivery. If this happens, call your gynaecologist urgently.
Finding and treating the cause of uncontrolled bleeding can lead to a full recovery. Recovery is different for everyone. Recovering from PPH depends on the severity of blood loss and how your doctor treats postpartum hemorrhage.
Successful obstetric hemorrhage bundle5 implementation is associated with improved outcome measures related to obstetric hemorrhage.
However, further research is necessary to evaluate better the particular effect of quantitative blood loss measurement in reducing maternal hemorrhage-associated morbidity in the United States.
- Rosenfeld, Cheryl S. “The placenta‐brain‐axis.” Journal of neuroscience research 99.1 (2021): 271-283. ↩︎
- Hegemann, Julian D., and Roderich D. Süssmuth. “Matters of class: coming of age of class III and IV lanthipeptides.” RSC Chemical Biology 1.3 (2020): 110-127. ↩︎
- Fuchs, Flávio D., and Paul K. Whelton. “High blood pressure and cardiovascular disease.” Hypertension 75.2 (2020): 285-292. ↩︎
- Wang, Ziyi, et al. “Mapping global prevalence of depression among postpartum women.” Translational psychiatry 11.1 (2021): 543. ↩︎
- Joseph, Naima T., et al. “Implementation of a postpartum hemorrhage safety bundle at an urban safety-net hospital.” American Journal of Perinatology Reports 10.03 (2020): e255-e261. ↩︎
Last Updated on by Suchi



