
 1")
Table of Contents Show
Welcome to the complete guide to Pancreatic Cancer Diagnosis and Treatment!
Cancer is a group of abnormal cells that can grow and spread to specific or whole parts of the body. Cancer cells divide uncontrollably and cause infection in the normal body tissue.
Pancreatic cancer develops when cancer cells grow in the pancreas, a small organ located in the lower part of the stomach and upper part of the large and small intestine. The pancreas’ primary function secrete enzymes that regulate blood sugar metabolism.
Pancreatic cancer cells can spread to other parts of the body. Pancreatic cancer can be detected late and spread quickly, but there are no symptoms of this type of cancer in its early stages.
Pancreatic enzyme products contain pancreatin or pancrelipase, a mixture of amylase, lipase, and protease that helps break down the starch, lipid (fats), and protein, respectively.
Six FDA-approved pancreatic enzymes are available by prescription only: Creon, Ultresa, Viokace, Pancreaze, Zenpep, and Pertzye.

In the central part of the pancreas, approximately 95% produces digestive enzymes such as lipase, protease, and amylase, known as exocrine components. Exocrine pancreatic cancers are the most common.
Whereas the hormone-producing tissue of the pancreas is known as pancreatic neuroendocrine, pancreatic neuroendocrine tumours are rare and have a small minority.
The early detection of pancreatic cancer is quite difficult, and people over 40, mainly men’s pancreatic cancer, can be detected. The most common pancreatic cancer accounts for 90% of the cases and is known as pancreatic adenocarcinoma.
Some risk factors for pancreatic tumours and cancer may include age, sex, obesity, smoking, and family history of cancer.
Some methods of pancreatic cancer diagnosis and treatment are discussed in this article.
Diagnosis of Pancreatic Cancer

Doctors may use a variety of tests to diagnose cancer, but it all depends on which part of the body is suspected of being cancerous.
A biopsy is the only way to determine if an area has cancer in most types of cancer. However, due to the location of the pancreas, biopsying pancreatic cancer is a difficult procedure.
Some standard tests to diagnose pancreatic cancer are blood tests, imaging tests, emission tomography pet scan, magnetic resonance cholangiopancreatography, percutaneous transhepatic cholangiography PTC, liver function tests, and computed tomography.
If a doctor suspects a patient has pancreatic cancer, the doctor will first inquire about their medical and family histories.
Diagnosing pancreatic cancer depends on the symptoms according to the location of the cancer in the pancreas which may be divided into the body, neck, thick head, and end in the pancreas’s tail.
For pancreatic cancer diagnosis, doctors use a variety of tests, but the results vary depending on the factors present during the examination;
- The patient’s age and family history
- The signs of cancer and the possibility of cancer
- The medical examination’s outcome
9 Diagnosis Tests for Pancreatic Cancer
If the doctor suspects pancreatic cancer, he will undergo lab tests, CT scans, imaging tests, and other tests.
1. Blood Test:
The doctor may take a blood tissue sample to check the level of the bile juice, which may reach a high level if the patient has pancreatic cancer. Carbohydrate antigen 19-9 (CA 19-9) is a tumour marker that suspects the tumours at a higher level if cancer is present.
This level is increased in people with pancreatic cancer, which a blood test can diagnose. These tumour markers also help understand how tumour tissue or cells respond to the treatment and targeted therapy.
2. Physical Examination:
The doctor can examine the skin and tongue. If they are yellow, then this is a sign of jaundice. However, it can be a form of tumour in the pancreas that can block the normal flow of bile and result in jaundice.
However, many people don’t have jaundice when cancer is diagnosed. The doctor can also check the upper abdomen; if the abnormal build-up is felt (ascites), it can be another sign of cancer.
3. Endoscopic Ultrasound:
Ultrasound can be used to create a picture of the internal organs. An endoscopic device is a light tube that passes through the mouth and slowly moves to the area around the pancreas to picture it.
The doctor inserts the tube into the patient’s mouth, passes through the endoscope and into the bile duct and pancreatic duct, and picturizes the blood vessels.
A gastroenterologist takes that test, and the patient sleeps throughout the process. Sometimes, a biopsy can also be done during an ultrasound procedure.
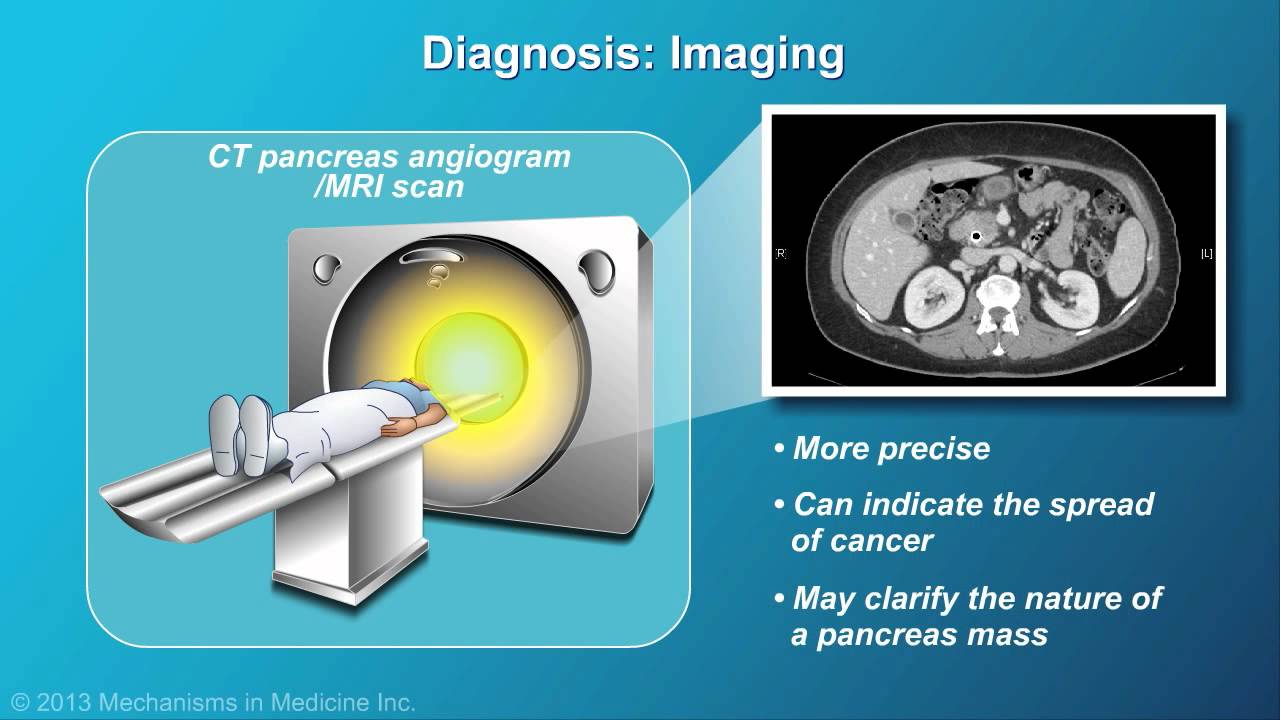
4. CT Scan:
A CT scan takes pictures inside the body using X-rays from different angles and gives 3D images that provide visibility of the cancer cells and tumours. A specialized Pancreatic protocol CT scan can be used to diagnose pancreatic cancer disease and treat it.
The cancer centres use the CT scan with IV injections to find where the tumour is growing in the nearby organ.
5. Endoscopic Retrograde Cholangiopancreatography:
This process is done under the instructions of the gastroenterologist and with the endoscope tube. This light and a small tube are passed through the mouth and into bile ducts and pancreatic ducts.
A sample of the tissues is taken during the procedure to confirm the cancer diagnosis. A dye is injected into the ducts, and doctors take an X-ray.
6. A Biopsy:
A biopsy is a procedure in which a fine needle aspiration is inserted into the pancreas to suction cells or tissue samples to obtain a tumour or a definitive cancer diagnosis.
A core needle biopsy can be used for tumour or cancer genetic testing, but it has the highest risk of bleeding.
7. Magnetic Resonance Imaging (MRI):
The magnetic resonance imaging test uses the magnetic field to produce an image of the body and measure pancreatic tumours.
A specific dye can be injected into the patients. MRI involves using computer software developed specifically to examine pancreatic cancer near the bile duct and pancreatic duct.
8. Positron Emission Tomography:
The PET scan combined with the CT scan is known as the PET-CT scan. This scanning is the most common procedure for the diagnosis of pancreatic cancer that produces multiple coloured pictures of organs, blood vessels, and tissue inside the body.
9. Biomarker Testing of the Tumour:
Doctors may suggest additional molecular tests to identify the specific mutation, genetic alteration, and molecular features of pancreatic cancer. A tissue sample may be sent to the lab for genetic testing. These types of tests may help the doctor determine the treatment options.
If the patient’s pancreatic cancer diagnosis is confirmed, the doctor will attempt to determine the cancer stage. The stages are denoted by the Roman numerals 0 through 4.
A zero stage indicates pancreatic cancer and a four-stage diagnosis indicates cancer that has spread to other body parts.
3 Types of Pancreatic Cancer Treatment
In cancer treatment, a team of doctors and health care professionals such as oncology nurses, physicians, social workers, patient navigators, and counsellors work together to provide the best treatment to the patient that combines the different types of treatment and care.
Some common treatments used for treating cancer are described here. Currently, the treatment option includes radiation therapy, immunotherapy, surgery, and chemotherapy.
The treatment of pancreatic cancer is dependent upon several factors, including the stage and the type of the cancer patient’s history, overall health, and possible side effects.
If pancreatic cancer is detected at an early stage, there are much higher chances for pancreatic cancer to be treated successfully.
1. Chemotherapy:
Chemotherapy treats cancer that hasn’t spread beyond the pancreas with radiation therapy and helps shrink the tumour before surgery. Chemotherapy uses drugs that kill cancer cells.
It may also use the injection or be taken orally to take the drugs. Chemotherapy helps control cancer growth and prolong the patient’s survival at stage 4.
The chemotherapy is scheduled for the patient for the period of time between the cycles. Chemotherapy may be prescribed by the doctor depending on the stage of cancer and the specific diagnosis.
The chemotherapy may be off-label chemotherapy or second-line, first-line chemotherapy to control the cancer growth, and it is off-label used and approved by the FDA.
There are often some side effects of chemotherapy depending upon the drugs the patient receives. Not all patients have the same side effects, but some common side effects are nausea, vomiting, hair loss, rashes, diarrhoea, low appetite, lack of energy, and low levels of RBC, WBC, and platelets.
The patients may receive a combination of the drugs at the same time. Some approved drugs for pancreatic cancers are-
- oxaliplatin
- Nanoliposomal irinotecan (onivyde)
- Nab-paclitaxel (abraxane)
- Fluorouracil (5-FU)
- Gemcitabine (Gemzar)
- Leucovorin (wellcovorin)
- Capecitabine (Xeloda)
2. Radiation Therapy:
Radiation therapy employs X-rays or protons to destroy cancer cells. Depending upon the doctor’s recommendation, patients may receive radiation therapy before or after cancer surgery.
If cancer can’t be treated surgically, the doctor may recommend a combination of radiation and chemotherapy treatments that may prolong the patient’s life and relieve cancer symptoms. Radiation therapy uses high-energy X-ray particles and is done under a radiation oncologist’s supervision.
Radiation therapy schedules for the number of times over a period. There are different ways that radiation therapy can be given to the patient with a specific schedule, such as traditional radiation therapy, also known as conventional radiation therapy, which is given as a low dose of radiation per day and given over 5 to 6 weeks from the treatment.
Stereotactic body radiation or cyberknife is a type of radiation therapy given over 5 days. They can be of shorter treatment or higher doses. They should be given in specialized centres for pancreatic cancer treatment options.
Radiation therapy is quite helpful for reducing the risk of pancreatic cancer regrowing or returning to its original position. Some side effects of radiation therapy may include nausea, mild skin reaction, allergy, or loose bowel movement.

3. Surgery:
Surgery for pancreatic cancer depends upon the tumour’s location or cancer in the pancreas. About 25% of people with pancreatic cancer may be able to have the surgery because most of the cancer is diagnosed when cancer has spread.
The doctor recommends the surgery after talking about the benefits, recovery time, risk factors, and the specific surgery depending upon the patient.
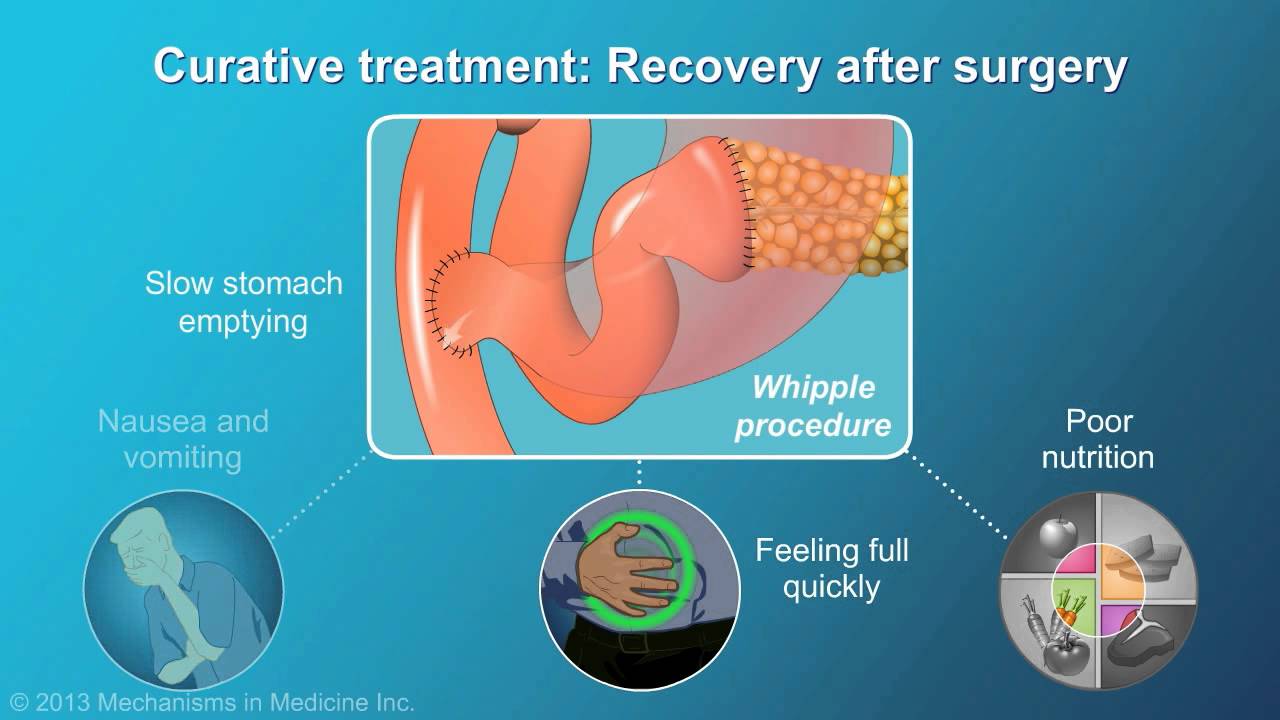
If the cancer is located in the head of the pancreas, the doctor recommends an operation called the Whipple procedure, which is used to remove the head of the pancreas, some part of the small intestine (duodenum), some part of the gallbladder, parts nearby lymph nodes, and the bile duct.
And the surgeon reconnects the digestive tract and the other systems. It is an extensive surgery in which the surgeon removes the head of the pancreas, also referred to as the pancreaticoduodenectomy.
Some common surgeries in the treatment options for pancreatic cancers or pancreatic tumours are distal pancreatectomy and total pancreatectomy.
Different types of surgeries are recommended by the doctor depending upon the pancreatic tumour location in the pancreas and how and where the pancreatic cancer action network is.
Systemic or radiation therapy may be given to the patient before the surgery to shrink that tumour, reducing complications during the surgery.
In some cases, if pancreatic cancer has spread all over the pancreas, the entire pancreas must be removed. This procedure is known as total pancreatectomy1. After this procedure, the patient must take lifelong insulin and enzyme replacement.
Side effects of pancreatic cancer surgery may include pain for the first few weeks after the surgery, weakness, and tiredness. If the total pancreas is removed during the pancreatic cancer surgery, there is difficult for the patient to digest the food and food metabolism2.
Mainly, pancreatic cancer is diagnosed at stage 4, and only up to 10% of patients can become disease-free after treatment if they are diagnosed with stage zero or one pancreatic cancer. It is potentially curable if diagnosed early, but if it is diagnosed at stage 4, cancer has grown and spread over the other organs.
In this case, the removal of the pancreas is the only treatment. The research estimates that pancreatic cancer spreads very easily in such a way that it takes only one year to reach the average stage one to four.
Network for Pancreatic Cancer
The National Comprehensive Cancer Network recommends genetic counselling for all pancreatic cancer patients. A genetic counsellor is a health professional who identifies the genetic cause of pancreatic cancer in the family.
Genetic counselling 3can help assess and navigate the treatment options for cancer prevention and tumour tissue prevention strategies. Currently, a cancer news push is close to the new therapy for pancreatic cancer by nanotechnology Cancer research.
The American Cancer Society is the best-known nationwide voluntary health organization dedicated to eliminating cancer and a global presence to ensure the mission of a cancer-free nation.
The American Cancer Society has increased pancreatic Cancer4 research funding to improve medical knowledge, diagnosis tests and treatment, and patient quality of life. The National Cancer Institute is working daily to make cancer issues a national priority and working on the principal agencies for Cancer research.
Currently, some clinical oncology trials and cancer research are being conducted to explore new treatments such as immunotherapy vaccines and chemotherapy drugs 5that can give a chance to try a new cure for pancreatic cancer.
The palliative care team is provided by doctors, social workers, and specially trained professionals for the patients to support them, make them feel better, and live longer.
Recurrence and Remission
The recurrence of pancreatic cancer may occur in or near the pancreas or elsewhere in the body, similar to metastasis. If pancreatic cancer recurs, a new cycle for pancreatic cancer is diagnosed.
During diagnosing pancreatic cancer, if there is a sign of cancer recurrence, the doctor may recommend some clinical trials to create recurrent cancer.
A diagnosis such as imaging tests, blood tests, endoscopic ultrasound, and tumour markers may be stressful and painful. Still, if the treatment doesn’t work, advanced cancer or terminal cancer6 is difficult.
Advanced cancer care can be made by the patient’s family, and special healthcare for people with pancreatic cancer who are expected to live for less than 6 months.
Key Takeaways
 3")
Pancreatic cancer is a devastating disease, but due to the poor outcome and current gaps in the knowledge, current cancer research makes the understanding of pancreatic Cancer disease better enables early diagnosis, and improves the treatment with the prolonged life of the patient.
Here, we have reviewed the current understanding of pancreatic cancer that must focus on the surgery, pathology, and radiation to the oncology treatment.
Molecular profiling and biobanking play an important part in pancreatic cancer research that improves the potential of translation research linked to pancreatic cancer treatment options.
FAQs
1. Which is the best treatment for pancreatic cancer?
Ans. CT Scan or Computed Tomography is the best treatment procedure for pancreatic cancer.
2. Is surgery really helpful in pancreatic cancer?
Ans. Surgery is actually the most successful treatment for pancreatic cancer, but only 20% of the cases respond well to surgery.
3. Which blood test is done to know if someone is suffering from pancreatic cancer?
Ans. Carbohydrate antigen 19-9 (CA19-9) indicates if someone is suffering from pancreatic cancer.
- Wu, Linda, et al. “Risk factors for development of diabetes mellitus (Type 3c) after partial pancreatectomy: a systematic review.” Clinical endocrinology 92.5 (2020): 396-406. ↩︎
- Leone, Robert D., and Jonathan D. Powell. “Metabolism of immune cells in cancer.” Nature reviews cancer 20.9 (2020): 516-531. ↩︎
- De Backer, Julie, et al. “Genetic counselling and testing in adults with congenital heart disease: A consensus document of the ESC Working Group of Grown-Up Congenital Heart Disease, the ESC Working Group on Aorta and Peripheral Vascular Disease and the European Society of Human Genetics.” European journal of preventive cardiology 27.13 (2020): 1423-1435. ↩︎
- Mizrahi, Jonathan D., et al. “Pancreatic cancer.” The Lancet 395.10242 (2020): 2008-2020. ↩︎
- Behranvand, Nafiseh, et al. “Chemotherapy: A double-edged sword in cancer treatment.” Cancer immunology, immunotherapy 71.3 (2022): 507-526. ↩︎
- Wajid, Maria, et al. “Why is hospice care important? An exploration of its benefits for patients with terminal cancer.” BMC Palliative Care 20.1 (2021): 70. ↩︎
Last Updated on by Suchi



