

Table of Contents Show
Miller-Fisher syndrome is a rare disorder, where the immune system of the affected individual attacks their nerves. Hence it is an autoimmune disorder. The disorder is a variant form of another rare disorder, Guillain–Barré syndrome.
1. What is an Autoimmune Disorder
The immune system can recognize and differentiate between the self and the non-self cells. This is because the immune system can recognize the antigens on the self cells, also called self-antigens.
Foreign substances like pathogens, pollen, chemicals, and toxins can all be considered antigens, and they are not recognized by the immune system. Hence the immune system generates a response against those foreign substances.
In an autoimmune disorder, the immune system cannot differentiate between self and non-self cells and attacks the self cells.

There are some factors linked to the genetics of an individual, which makes him/her/them more prone to develop an autoimmune disorder as compared to other individuals. If an individual has these genetic factors, it does not mean that he/she/they will develop an autoimmune disorder, the presence of the factors simply means that they are more susceptible to developing the disorder.
Some reports have even suggested that the sex of the individual may also play a role in developing an autoimmune disorder. Many of these disorders occur more frequently in people of one sex as compared to people of the other sex. Hashimoto’s thyroiditis is one such autoimmune disorder that occurs more frequently in women as compared to men.
The ratio of incidence for this disorder is 10:1 (female: male). Another such disorder is Graves’ disease. This autoimmune disorder occurs more frequently in females as compared to males. The ratio of incidence for this disorder is 7:1 (female: male). Some of the disorders that occur in almost the same frequency in both sexes are psoriasis and Crohn’s disease.
2. What are Antigens?
Any substance or molecule which elicits an immune response against it, or simply put, causes the immune system to generate antibodies against it, they are called an antigen. There can be various types of antigens that affect an individual, and they can be living as well as non-living molecules. Some examples of these antigenic substances can be pathogens, pollens, toxins, and some kinds of chemicals.
It is important to understand here that not all antigens are capable of triggering the immune system to generate a response against them. There are some factors that an antigen must possess to elicit a response from the immune system.
If the foreign substance or molecule is successful in eliciting a response from an organism’s immune system, it is considered to be an immunogen. Every immunogen is an antigen that was able to trigger an immune response.
2.1 Immunogen
Various factors that a molecule must possess for being immunogenic are the foreignness of the molecule, the size of the molecule, and the chemical complexity of the molecule. Some antigens are unable to elicit an immune response against them as they lack some of these factors.
For example, haptens are antigenic molecules but they are unable to trigger an immune response against them, because of their small size. These molecules are not immunogenic. Hence not every antigen can be considered to be an immunogen.
So precisely, an antigen is such a substance that may or may not be able to elicit a response from the immune system, but if the response against them is generated by some mechanism, the antigen can react with or combine with the products that have been generated by this response.

2.2 Substances That Act Like Antigens
Various substances or molecules that can act as antigens are proteins, polysaccharides, peptides, lipids as well as nucleic acids. The combination of these substances or molecules, for example, lipopolysaccharides, can also act as antigens for an organism.
In the case of pathogens, their cell walls, surface proteins, coat, capsule, and the toxins they release can all act as antigens. The antigens can also be generated inside the organism, and these are called self-proteins. The body has some mechanism, through which it avoids interacting or reacting with these self-proteins.
After an immune response is generated against them, the antigens are recognized by antigenic receptors, and these receptors include antibodies and T cell receptors or TCR. The receptors have specificity for an antigen.
After an antigen enters the body of an organism and elicits an immune response, lymphocytes that are specific for that antigen are activated and this phenomenon is clonal selection. After activation, those specific lymphocytes are proliferated and this phenomenon is clonal expansion.
3. What is Guillain–Barré syndrome?
Miller-Fisher syndrome is considered a subtype of a disorder called Guillain–Barré syndrome. GBS is a rare neurological disorder. In this disorder, the immune system attacks the peripheral nervous system of the affected individual. It is characterized by weakness of the muscles.
The nervous system which consists of components like nerves and ganglia, forms the peripheral nervous system. The peripheral nervous system is involved in important functions in the body. It consists of carrying signals from different parts of the body to the brain as well as carrying commands from the brain which are then passed on to follow, the rest of the body.
Two main types of the peripheral nervous system can be categorized into the autonomic and the somatic. The somatic functions involve thinking while in the case of autonomic functions, they do not require any thinking and are done automatically by the brain.
As it is an autoimmune disorder, the cause of this disorder is not known. The trigger for this disorder can be a viral infection or a bacterial infection. Some other less common triggers for this disorder can include surgery and vaccination. GBS is not passed down through the generations, hence it is not an inherited disorder. The disorder is also not contagious
3.1 Miller-Fisher Syndrome
Miller-Fisher syndrome is considered a subtype of this disorder. Guillain–Barré syndrome has many subtypes other than just Miller-Fisher syndrome.
In the subtype Pharyngeal-cervical-brachial variant, the antiganglioside autoantibodies that commonly occur are GT1a. Antiganglioside autoantibody that occurs with less frequency in this variant is GQ1b. Another antiganglioside autoantibody that occurs rarely in this disorder is GD1a. Some of the symptoms that are observed in this subtype of Guillain–Barré syndrome are a weakness of the throat muscles, weakness in the face muscles, and weakness in the shoulder muscles.
Till now, there is no specific ethnicity, sex or age reported that has more occurrence of this subtype relative to others.
3.2 Symptoms
In the subtype Miller Fisher syndrome, the antiganglioside autoantibodies that commonly occur are GQ1b and GT1a. Some of the symptoms that are observed in this subtype of Guillain–Barré syndrome are ataxia, areflexia, weakness of the eye muscles, and no weakness in limb muscles. This subtype occurs more frequently in males as compared to females.
In the subtype of Acute motor axonal neuropathy, the antiganglioside autoantibodies that commonly occur are GM1a/b, GD1a as well as GalNac-GD1a. Some of the symptoms that are observed in this subtype of Guillain–Barré syndrome are muscle weakness but without any sensory observations, and it occurs in less than 10% of the affected people.
Around 30% to 65% of the cases are located in Asia, Central America, and South America. Another name by which the disorder might be referred is Chinese paralytic syndrome.
Some of the common symptoms of GBS include
- Numbness or a tingling sensation that occurs in the hands or feet
- Difficulty in breathing due to the breathing muscles becoming weak can cause respiratory failure
- Difficulty in swallowing
- Muscle weakness like face muscle weakness, and eye muscle weakness.
3.3 Diagnosis
The diagnosis of Guillain–Barré syndrome can be done by various techniques, and through diagnostic tests and imaging, it is important to confirm that the person is not affected by any other disorder which might present similar symptoms like spinal cord compression.
Blood tests can be done for patients who are suspected to be suffering from Guillain–Barré syndrome. In such patients, there will be an abnormal reduction in the levels of sodium in their blood. Blood testing can also be used for verification of the disorder, as after blood tests if low levels of potassium are found in the blood sample, it can be a cause of weakness.

Cerebrospinal fluid can also be tested for patients who are suspected to be suffering from Guillain–Barré syndrome. A spinal tap is performed to isolate the spinal fluid sample for further testing. In patients who are suffering from Guillain–Barré syndrome, an increased level of protein will be observed in their spinal fluid samples.
Albuminocytological dissociation is considered to be a characteristic observation in a spinal fluid sample of patients with Guillain–Barré syndrome. One important point to take care of is that it is not advised to go through the spinal tap again during the period when suffering from the disorder, as after the patient has been given some treatment, there is a possibility of the protein levels rise, which can give some false results.
4. What is the Cause of Miller-Fisher Syndrome?
It is an autoimmune disorder where the immune system of the individual attacks the nerve. Some proteins are present on the nerves which are responsible for movement, sensation as well as function, and these proteins are attacked by the individual’s immune system. After a bacterial or viral illness, the antibodies, that were generated in response to the antigens of these pathogens, start to attack proteins on the nerves.
It is suggested that molecular mimicry between the antigens of the peripheral nerves and the bacterial or viral antigen occurs through adaptive immune system activation. Molecular mimicry is considered to be one of the possible mechanisms of how infection or some chemical agents can cause an autoimmune disorder. In this mechanism, there are some sequence or structural similarities between the foreign antigen and the self-antigen.

The foreign antigen activates the adaptive immune response. It consists of T lymphocytes and B lymphocytes. Although the T and B cells were generated for the foreign antigen, the similarity between the foreign and self-antigen causes cross-reactivity of self-antigens with autoreactive B and T cells.
Multiple studies have suggested that IgG anti-GQ1b antibody, an autoantibody that is produced by the body against ganglioside GQ1b, is a specific characteristic of Miller-Fisher syndrome. Other sites that can be attacked are myelin sheaths or axons.
Miller-Fisher syndrome usually occurs after an infection. The duration can be several days to weeks up to four weeks. The most common bacteria that acts as a trigger for the disorder is Campylobacter jejuni, which can cause diarrhea and pain in the abdomen.
Another bacteria that commonly acts as a trigger is Haemophilus influenza, which can cause infections of the respiratory system, like pneumonia, and epiglottitis.
Some viruses that can act as triggers are HIV, Zika virus, and Epstein-Barr.
5. Who is Affected by Miller-Fisher Syndrome?
Miller-Fisher syndrome occurs in both men and women of all ages. But, it occurs more commonly in men as compared to women, approximately twice as more than women. The disorder occurs more commonly in people from East Asia.
The average age when the disease occurs is 45 years. Every year, around the globe, Miller-Fisher syndrome affects only one to two per million people.
6. What are the symptoms That Occur in Miller-Fisher Syndrome?
Some of the common symptoms of Miller-Fisher syndrome are:
6.1 Ophthalmoplegia
It is an eye disorder, and can also be referred to as extraocular muscle palsy. Weakness or paralysis of one or multiple extraocular eye muscles occurs. These muscles played a role in the control of eye movements. Impaired movement of the eye and double vision can occur due to weakness of the eye muscles.
6.2 Ataxia
It is characterized by an impaired balance or coordination of the movement of voluntary muscles.
6.3 Areflexia
It is characterized by the absence of tendon reflexes. Tendons are involved with the connection of muscles to bones. Normally, when an individual’s tendon is tapped, there is an involuntary movement which is caused by muscle contraction. One such common example is tapping the side of the knee which can cause the leg to move up involuntarily.

These tendon reflexes can be observed in other parts of the body as well like the elbow, and ankle. If the tendon reflex is absent, it can be a symptom of problems with the nerves that are present in the tendon and the muscle.
Other symptoms include
- Numbness or tingling that occurs in the feet or hands.
- Pain in the arms, legs, and back
- Develop weakness of the facial muscles
- Weakness of tongue and swallowing muscles
- Decreased gag reflex
- Weakness of breathing muscles can lead to breathing problems.
- Blurred vision
7. How is Miller-Fisher Syndrome diagnosed?
It is difficult to diagnose Miller-Fisher syndrome as many other neurological disorders have some similarities with Miller-Fisher syndrome. Some of these neurological disorders include botulism, myasthenia gravis, and basal meningitis.
Symptoms of the disorder can be observed in the patient and a physical examination can be performed, along with reviewing the patient’s medical history. But a physical exam may not be enough, and some tests have to be performed to verify that the disorder in the patient is Miller-Fisher syndrome and not any of the similar disorders.
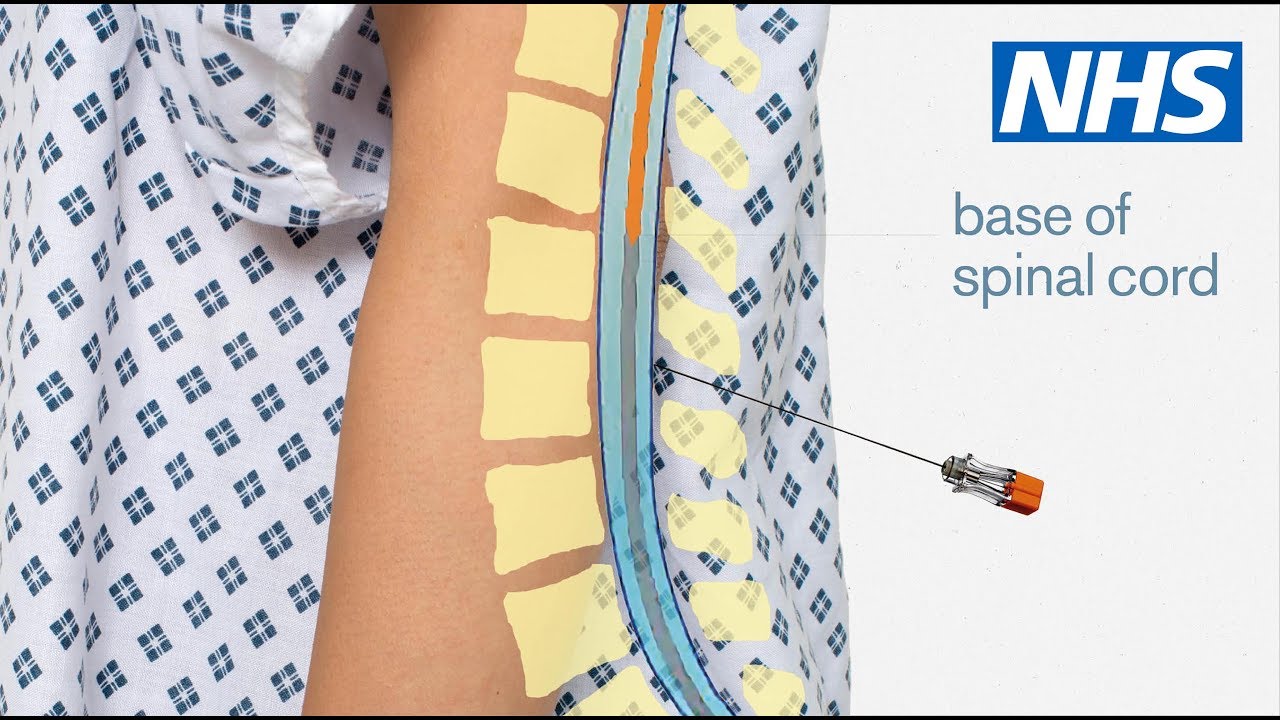
7.1 Spinal tap
It is also called a lumbar puncture. Using a thin hollow needle is inserted in the lower back of the patient and a sample of cerebrospinal fluid is withdrawn. Further testing can be performed using the sample, like testing for types and levels of protein and testing for glucose levels.
Many people with Miller-Fisher syndrome have high levels of proteins in their spinal fluid.
7.2 Blood test
The blood sample of a person can be checked for the presence of anti-GQ1b antibodies. Though these antibodies are commonly present in people with Miller-Fisher syndrome (about 95%), it is not present in every patient.
The presence of these antibodies does not definitively prove Miller Fisher syndrome as these autoantibodies can also occur in Bickerstaff brainstem encephalitis. In Miller-Fisher syndrome, the cell count is normal while, in one out of three patients of Bickerstaff brainstem encephalitis, the cell count is increased.
These blood tests can also be performed to make sure that some of the other diseases are not present.
7.3 Electromyography and Nerve Conduction Study
EMG can be used for measuring electrical activity which is a response by the muscles on being stimulated by a nerve. In this diagnostic test, electrodes, which are small needles, are inserted into the muscle. An oscilloscope can then be used to display the electrical activity that was detected by the electrodes.
Through electromyography, for Miller-Fisher syndrome, we can diagnose whether the response of the muscle to the nerve is correct or not.
NCS is a diagnostic test that is used to evaluate the electric conduction by the sensory nerves as well as motor nerves. The test can measure the speed of the electric impulse that travels through the nerve. The test can be used for the detection of nerve damage and can evaluate if the nerves are carrying the electrical signals correctly.
In Miller-Fisher syndrome, the tests conducted for motor nerve tests yield a normal result. For sensory nerves, there are abnormalities detected and the sensory nerve action potential is absent.
7.4 Imaging Techniques
Magnetic resonance imaging of the brain can be performed. In the case of Miller-Fisher syndrome, the MRI turns out to be normal. But in the case of other disorders, there can be brain abnormalities observed and thus can be used to rule out the other disorders. One such example is Bickerstaff brainstem encephalitis, in which the brain stem shows abnormalities.
The imaging tests can also be used for the spine, where the tests can detect if the immune system is attacking the nerves in the spinal cord.
8. What are the treatments available for Miller-Fisher Syndrome?
There is presently no cure for Miller-Fisher syndrome but the symptoms can be treated or managed.
The treatment for patients with Miller-Fisher syndrome is often done in hospitals to manage any severe or life-threatening complications due to the disorder. If severe breathing issues develop in the patients, a breathing tube is required.
Plasmapheresis, which can also be referred to as plasma exchange, can be used for treatment. A thin plastic tube helps in connecting the vein to the machine. The blood of the patient is passed through this machine which separates the blood from plasma. A replacement fluid is added to the blood and the blood is returned by the body of the patient.
The autoantibodies that were attacking the nervous system are removed. It is performed about five times over two weeks.

Intravenous immunoglobulin therapy or IVIG is one of the initial treatments for patients because it is more convenient and more broadly available as compared to plasmapheresis. Immune globulins are obtained from pooled plasma of many healthy people and are highly purified.
High doses of these immune globulins are infused into the veins of the patients. immunoglobulin therapy is thought to function by blocking the effects of those antibodies that are responsible for the disorder. It is performed every day for five days.
Physical therapy might be required by most patients whose muscles have been weakened by the disorder. The majority of people recover from Miller-Fisher disorder in about six months. The average duration for recovery from this disorder is around 8 weeks to 12 weeks. Death occurs rarely and the rate of recurrence for the disorder is less than 3%.
9. Conclusion
In conclusion, Ophthalmoplegia, ataxia, and areflexia are the primary symptoms of Miller-Fisher Syndrome (MFS), a rare variation of Guillain-Barré Syndrome (GBS). Infections are frequently implicated in their etiology, and early detection is key to better outcomes. Supportive care and immune-modulating treatments are part of the treatment. The vast majority of people heal on their own. To better understand and manage MFS, research must continue.
Along with all treatment measures, the patients should be given psychological support, and the patients should be given complete information regarding the disorder.
Last Updated on by Sparsh Sehgal



