

Table of Contents Show
The thyroid is a butterfly-shaped gland located in the neck, wrapped around the trachea. It is pivotal in the body’s proper metabolism1, body temperature, growth, and development. The thyroid cells responsible for the production and secretion of thyroid hormones are the Thyroid follicular cells.
Thyroid cancer is cancer in which abnormal cells grow in the normal thyroid cells of the thyroid gland. It might have the potential to spread to different parts of the body.
1. Major Types Of Thyroid Cancer:
According to the National Comprehensive Cancer Network (NCCN), different types of thyroid cancers can start in the thyroid gland. With surgery and treatment, the common types of thyroid cancer 2are curable.

Listed below are the most common types of thyroid cancer you should know about:
1.1. Papillary Thyroid Cancer
The most common type of thyroid cancer, Papillary Thyroid Cancer is mostly seen in women whose age is between early adulthood and late fifties. This thyroid cancer grows slowly, in only one lobe of the thyroid gland, although it might metastasize (most commonly to lymph nodes.3)
On routine examination, Papillary Thyroid Carcinoma is identified as an asymptomatic mass of thyroid nodules on the neck, normally referred to as fine-needle aspiration biopsy (FNA) for investigation purposes. In some instances, the mass can produce local symptoms.
Treatment:
The foremost treatment for papillary carcinoma4 is surgery. According to The Revised 2009 American Thyroid Association guidelines, state that the initial procedure for papillary thyroid cancer should be near-total or total thyroidectomy.
Under given circumstances, for small (<1 cm), low-risk, unifocal, intrathyroidal papillary carcinomas5, thyroid lobectomy 6alone may be sufficient treatment. It is one of the well-differentiated cancers.
Papillary thyroid cancer incidence is high, representing around 90% of all diagnosed thyroid cancers.
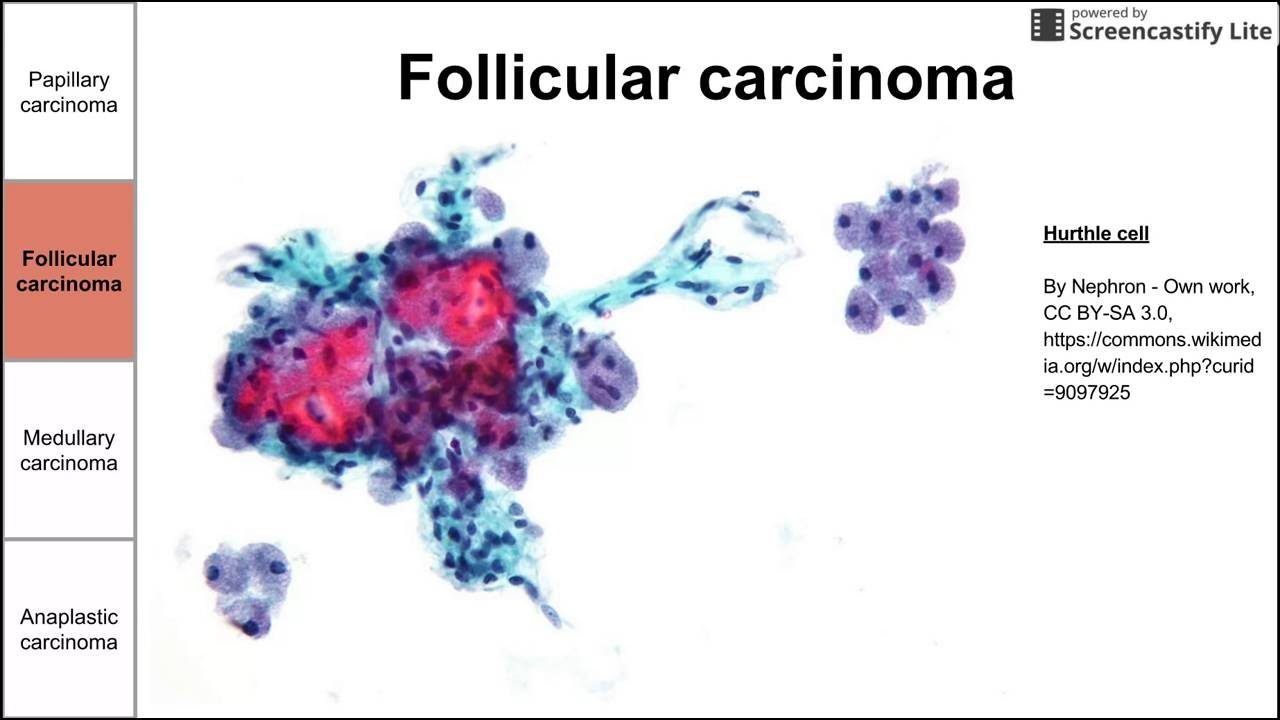
1.2. Follicular Thyroid Cancer

Follicular thyroid carcinoma is the second most common type of thyroid carcinoma which affects the follicular cells. It occurs most commonly in women between the age of 50 and above. Not getting enough iodine due to lack of a healthy diet is a cause of Follicular Thyroid Cancer.
Follicular thyroid cancer is one of the many low-risk, well-differentiated thyroid cancers. Mostly Thyroglobulin is used as a tumor marker for follicular thyroid cancers.
1.2.1. Follicular Thyroid Cancer: Hürthle Cell Carcinoma
Hurthle cell cancer is a variant of follicular cell carcinoma. It is also known as Oxyphil Cell Carcinoma7. Unlike the follicular type of thyroid cancer, the Hurthle cell carcinoma forms are mostly bilateral and multifocal and metastasize to lymph nodes.
Treatment:
Like follicular carcinoma, unilateral hemithyroidectomy is performed for non-invasive Hürthle cell disease and total thyroidectomy for invasive Hürthle cells disease.8
1.3. Medullary Thyroid Cancer
Medullary Thyroid Cancer is a well-differentiated thyroid cancer that originally affects the C cells or the parafollicular cells. Medullary thyroid Carcinoma may also produce a thyroid nodule and enlarged cervical lymph nodes in some thyroid cancer patients.
There can also be Familial MTC which can’t always be predicted through DNA testing. The germline mutation of RET is responsible for the genetic syndromes of all almost all cases of familial Medullary Thyroid Cancer.
Treatment:
Surgical removal of the thyroid gland with the mutant gene in children is curative if the entire thyroid gland can be removed, before the spread of the thyroid tumors.
Medullary Thyroid Cancer is lesser differentiated thyroid cancer with an incidence of 3-4% of all thyroid cancer types each year in the U.S.
1.4. Anaplastic Thyroid Cancer
Characterized by the inexorable growth of cancer cells in normal thyroid tissue, Anaplastic thyroid carcinoma is one of the aggressive forms of thyroid cancer. Because Anaplastic thyroid cancer does not grow slowly, persistently harms normal cells, and resists cancer cells treatments, its prognosis is generally low.
Treatment:
Several ATCs have non-differentiated cancers to differentiated thyroid cancer cases and hence aggressive and difficult to treat. The 5-year survival rate for these types of thyroid cancer is low.
Other factors that affect prognosis include the person’s metabolism, age, the presence of metastases, the dose of radiation administered to the primary tumor and surrounding lymph nodes, and if combined modality treatment is used.
Differentiated cancers of the thyroid gland are seen coexisting with Anaplastic thyroid cancer on fine-needle aspiration biopsies in 20-50% of thyroid cancer cases.
2. Rare Types of Thyroid Cancer:

Clinical Oncology and Clinical Endocrinologists at the National Cancer Institute identify several rare forms of thyroid cancer which affect healthy thyroid cells and hence the body’s endocrine system. Some of such thyroid malignancies and benign cancers are listed below:
2.1. Multiple Endocrine Neoplasia
Multiple Endocrine Neoplasia is an umbrella term for several distinct tumors (neoplasia) in at least two endocrine glands of the body. These tumors or thyroid nodules can be noncancerous i.e., benign or cancerous, malignant or fatal. It is a rare type of thyroid cancer.
MEN can be distinguished into type 1, type 2, and type 4 depending upon the genes involved, the types of hormones made, and the characteristic symptoms.
2.1.1. Symptoms:
Type 1 often includes tumors of the parathyroid glands, the pituitary gland, and the pancreas whereas the most common sign of Type 2 MEN is Medullary Thyroid Cancer. Some people may also develop pheochromocytoma which causes dangerously high blood pressure.
2.2. Thyroid Lymphoma
A rare form of thyroid cancer, Thyroid Lymphoma predominantly affects females over the age of 70 years and those with a history of Hashimoto’s Thyroiditis9 in particular. This type of thyroid cancer manifests itself as a rapidly enlarging neck mass of cancer cells which often compress the nearby trachea, causing breathing difficulties or in severe cases, respiratory failure.
2.2.1. Symptoms:
People affected with this type of thyroid cancer typically exhibit a firm thyroid gland and enlarged lymph nodes, since the cancer cells spread to lymph nodes.
Because it is one of the rare thyroid cancer types, Thyroid Lymphoma is difficult to diagnose. This is primarily because its syndrome is similar to Anaplastic Carcinoma. Fine-needle Aspiration may help distinguish the two differentiated thyroid cancers.
2.3. Undifferentiated Thyroid Carcinoma
Undifferentiated Thyroid Carcinoma, also called Undifferentiated Carcinoma is cancer arising from the follicular thyroid epithelium.
2.3.1. Symptoms:
However, it lacks the typical differentiation feature of the thyroid gland, like iodine uptake, thyroglobulin secretion, and response to TSH stimulation. These are the most aggressive types of thyroid malignancy.
Types of Thyroid Cancer: More information

The thyroid is integral in the human body and hence thyroid cancer afflicting normal thyroid cells immune system cells in some cases and other parts of the body should be coped with. Most differentiated cancers of the thyroid are not fatal.
One can know more about the types of thyroid cancer by researching thyroid cancer on platforms like The National Cancer Institute, and The American cancer society, or by acquainting the NCCN Clinical Practice Guidelines on types of Thyroid cancer. Abeloff’s Clinical Oncology will be a useful read in this regard.
Click here to read more.
Reviewed by: Omejua Chimdike (B.MLS), Biomedical Scientist (UNN)
About Omejua Chimdike .G.
A talented, knowledgeable and certified medical laboratory scientist with experience in carrying out standard laboratory practices (tests) on patients of various cultural backgrounds with the aim of researching and developing diagnostic approaches that will aid in the diagnosis of diseases and increase patient outcomes to treatment. Currently, working as a research scientist at Everight Diagnostic Laboratory Services limited (Centre for Research and Molecular Studies), Nigeria.
LinkedIn: https://www.linkedin.com/in/chimdike-omejua-520859199
WordPress : https://omejuachimdikeacademia.wordpress.com/
Gmail: chimdike.omejua.188155@unn.edu.ng
- Appel, Jens, and Rüdiger Schulz. “Hydrogen metabolism in organisms with oxygenic photosynthesis: hydrogenases as important regulatory devices for a proper redox poising?.” Journal of Photochemistry and Photobiology B: Biology 47.1 (1998): 1-11. ↩︎
- Gimm, Oliver. “Thyroid cancer.” Cancer letters 163.2 (2001): 143-156. ↩︎
- Willard-Mack, Cynthia L. “Normal structure, function, and histology of lymph nodes.” Toxicologic pathology 34.5 (2006): 409-424. ↩︎
- Pal, Sumanta Kumar, et al. “Papillary carcinoma of the breast: an overview.” Breast cancer research and treatment 122 (2010): 637-645. ↩︎
- Vickery Jr, Austin L., Chiu‐An Wang, and Alexander M. Walker. “Treatment of intrathyroidal papillary carcinoma of the thyroid.” Cancer 60.11 (1987): 2587-2595. ↩︎
- Matsuzu, Kenichi, et al. “Thyroid lobectomy for papillary thyroid cancer: long-term follow-up study of 1,088 cases.” World journal of surgery 38 (2014): 68-79. ↩︎
- Young, Robert H., and Robert E. Scully. “Oxyphilic Clear Cell Carcinoma of the Ovary A Report of Nine Cases.” The American journal of surgical pathology 11.9 (1987): 661-662. ↩︎
- Cannon, Jennifer. “The significance of Hürthle cells in thyroid disease.” The oncologist 16.10 (2011): 1380-1387. ↩︎
- Ragusa, Francesca, et al. “Hashimotos’ thyroiditis: Epidemiology, pathogenesis, clinic and therapy.” Best Practice & Research Clinical Endocrinology & Metabolism 33.6 (2019): 101367. ↩︎
Last Updated on by ayeshayusuf



