

Table of Contents Show
The signs and symptoms of retinal detachment 1may be at higher risk. Retinal detachment surgery2 is used to repair circulation to the retina and maintain vision. Retinal detachment is a critical condition of the eye in which the retina stops receiving oxygen. Objects would seem to float throughout your eye, or a gray veil may also move across your area of vision.
If they are no longer treated quickly, a retinal detachment can cause you to lose your vision. If you have the signs and symptoms defined above, you must call your ophthalmologist or visit the emergency department immediately.
1. Retinal Detachment Surgery

If you have a retinal detachment, you could need retinal detachment surgery to reattach your retina to the back of your eye within some days. After the surgery of a detached retinal, you may want to stay withinside the hospital for a short time — and it would take some weeks earlier than your vision starts getting better.
There are three forms of surgery that medical doctors can do to fix a detached retina:
In the type of retinal detachment surgery for retinal detachment, you will rely on numerous things, including how much of your retina is detached and where it is detached in your eye. Your medical doctor will communicate to you about what type they recommend and the dangers and advantages of surgery. Some humans may also want multiple types of surgery at once.
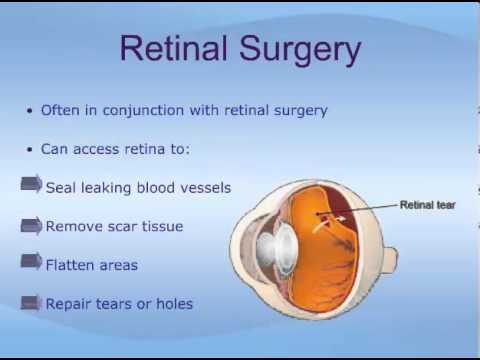
During the surgical procedure, your surgeon might also use laser or freeze remedies to restore retinal tears or holes to your retina and assist keep your retina in place after surgery.
2. How Is Retinal Detachment Surgery Repair?
2.1. Pneumatic Retinopexy
Pneumatic retinopexy describes the injection of a gas bubble into the vitreous area inside the eye, permitting the gas bubble to push the retinal tear back in opposition to the wall of the eye and near the tear. Laser surgery or cryosurgery secures the retina to the eyewall across the retinal tear.
Your ophthalmologist will ask you to keep a specific head position for numerous days. The gas bubble will steadily disappear. Sometimes this method may be executed in the doctor’s office.
2.2. Scleral Buckle
A scleral buckle or flexible band is positioned across the eye’s equator to counterbalance any force pulling the retina out of place. This method is done in the operating room, general outpatient. Often the ophthalmologist will drain the fluid from under the detached retina, permitting the retina to go back to its ordinary position in opposition to the back wall of the eye.
2.3. Vitrectomy
A vitrectomy is a retinal detachment surgery to put off the vitreous gel that pulls on the retina. This will also be vital if the vitreous is replaced with a gas bubble. Your body’s fluids will progressively replace this gas bubble; however, the vitreous gel does now no longer returns. Sometimes a vitrectomy can be combined with a scleral buckle.
2.4. Laser Surgery (Laser Photocoagulation)

Laser (thermal) therapy or cryopexy (freezing).6 Sometimes, your provider will diagnose a retinal tear earlier than the retina starts pulling away. Your provider uses a medical laser or a freezing tool to seal the tear. These devices create scar tissue that holds the retina in place.
5. Symptoms Of Retinal Detachment

If only a tiny part of your retina has detached, you could no longer have any symptoms. But if more of your retina is detached, you can no longer be able to see as clearly as normal, and you may observe different unexpected signs and symptoms, including:
- A lot of new floaters (small darkish spots or squiggly lines that flow throughout your vision)
- Flashes of light in a single eye or both eyes
- A dark shadow or “curtain” on the edges or withinside the center of your field of vision
Retinal detachment surgery is a medical emergency. If you have signs and symptoms of a detached retina, it’s essential to visit the retina specialists or the emergency room.
The signs and symptoms of retinal detachment frequently come on quickly. If the retinal detachment isn’t dealt with properly away, more of the retina can detach, increasing the danger of permanent vision loss or blindness7.
6. Retinal Detachment Types
6.1. Rhegmatogenous

Rhegmatogenous8 is the most common kind. It occurs due to a retinal tear. You can also have it due to an eye injury, surgery, or nearsightedness. Age generally causes it because the vitreous gel that fills your eyeball pulls away from your retina.
6.2. Tractional

This kind takes place while scar tissue pulls in your retina, generally because diabetes has damaged the blood vessels withinside the back of your eye.
6.3. Exudative

This type takes place while fluid builds up in the back of your retina; however, there’s no tear. The fluid pushes your retina far from the tissue at its back. Common causes consist of leaking blood vessels and swelling due to conditions that include an injury, inflammation, or age-related macular degeneration.
7. How Is Retinal Detachment Diagnosed?

You want an eye examination to diagnose retinal detachment. Your eye care provider will use a dilated eye examination to test your retina. They’ll put eye drops on your eyes. The drops dilate or widen the pupil. After some minutes, your provider can get a close examine the retina.
Your provider may also suggest different tests after the dilated eye examination. These tests are noninvasive and won’t hurt. They assist your provider see your retina clearly and in more detail:
- Optical coherence tomography (OCT): You get eye drops for your eyes. Then you sit ahead of the OCT machine. You relax your head on a support, so it remains still. The machine scans your eye but doesn’t touch it.
- Eye (ocular) ultrasound: You won’t need to dilate drops for this test; however, your provider may also use drops to numb your eyes so that you won’t experience any discomfort. You sit in a chair and relax your head on a support, in a certain position.
Your provider gently places a device in opposition to the front of your eye to scan it. Next, you sit with your eyes closed. Your provider places gel on your eyelids. You circulate your eyeballs as your eye surgeon scans them with the equal instrument with your eyes closed.
8. What Are The Results Of Retinal Detachment Surgery?

Retinal detachment surgery is successful in approximately 85% of patients with a single vitrectomy or scleral buckle procedure. With additional surgical treatment, over 95% of retinas are reattached successfully. However, several months may also pass before the vision returns to its last level. The last outcome for vision relies upon numerous factors. For example, if the macula becomes detached, central vision not often will go back to normal because of degenerative changes withinside the macula.
The visual changes, in this case, are just like the ones visible with a lot more common condition referred to as macular degeneration. Even if the macula was now no longer detached, a few visions might still be lost, even though the maximum can be regained. New holes, tears, or pulling may also develop main to new retinal detachments. There can be scarring because of subretinal fibrosis9.
If gas or air bubble becomes inserted into the eye throughout retinal detachment surgery, preserving the right positioning of the head is likewise essential in figuring out the outcome. Pars plana vitrectomy and the usage of intraocular gas in phakic eyes are related to the subsequent excessive incidence of cataracts.
9. Conclusion
Successful retinal detachment surgery relies upon the seriousness of the tears and detachment and what sort of scar tissue was formed withinside the retina. Vision can be good if the macula or central part of the retina is no longer affected.
If the macula was detached for a long time, some vision would return, however, it’ll frequently be less than 20/200, which is legally blind. It may also take numerous months of recovery after surgery to decide how much vision will return.
Therefore, close follow-up through an ophthalmologist is needed, and visits will consist of the slit-lamp exam and dilated exam of the retina and vitreous. Because of the expanded hazard of retinal detachment withinside the other eye, dilated examination of the non-operated eye can also be performed.
Long-time period research has proven that even after preventive remedy of a retinal hole or tear, 5%-14% of patients may also increase new breaks within the retina, resulting in a retinal detachment.
Overall, however, repair of retinal detachments has made superb strides withinside the past twenty years with the recovery of healthy vision to many hundreds of people.
FAQs
1. Are there any risks or complications associated with the surgery?
A. Like any surgical procedure, retinal detachment surgery carries some risks. Potential complications may include infection, bleeding, cataract formation, increased intraocular pressure, or recurrent detachment. It’s essential to discuss these risks with the surgeon before undergoing the procedure.
2. Are there any restrictions or precautions after surgery?
A. Patients are typically advised to avoid activities that may strain the eyes, such as heavy lifting, vigorous exercise, and bending over, during the early stages of recovery. Additionally, they may need to use eye drops and attend follow-up appointments to monitor the healing progress.
3. Can retinal detachment recur after surgery?
A. In some cases, retinal detachment can recur after surgery. The risk of recurrence depends on various factors, including the initial cause of the detachment, the success of the surgery, and the patient’s overall eye health. Regular eye check-ups are essential to catch any potential issues early.
Read more
- Gariano, Ray F., and Chang-Hee Kim. “Evaluation and management of suspected retinal detachment.” American family physician 69.7 (2004): 1691-1699. ↩︎
- Schwartz, Stephen G., Harry W. Flynn Jr, and William F. Mieler. “Update on retinal detachment surgery.” Current Opinion in Ophthalmology 24.3 (2013): 255-261. ↩︎
- Chan, Clement K., et al. “Pneumatic retinopexy for the repair of retinal detachments: a comprehensive review (1986–2007).” Survey of ophthalmology 53.5 (2008): 443-478. ↩︎
- Wang, Aijing, and Martin P. Snead. “Scleral buckling—a brief historical overview and current indications.” Graefe’s Archive for Clinical and Experimental Ophthalmology 258 (2020): 467-478. ↩︎
- Thompson, John T. “Advantages and limitations of small gauge vitrectomy.” Survey of ophthalmology 56.2 (2011): 162-172. ↩︎
- Veckeneer, Marc, et al. “Randomized clinical trial of cryotherapy versus laser photocoagulation for retinopexy in conventional retinal detachment surgery.” American journal of ophthalmology 132.3 (2001): 343-347. ↩︎
- Sardegna, Jill, and Susan Shelly. The encyclopedia of blindness and vision impairment. Infobase Publishing, 2002. ↩︎
- Sodhi, Akrit, et al. “Recent trends in the management of rhegmatogenous retinal detachment.” Survey of ophthalmology 53.1 (2008): 50-67. ↩︎
- Ishikawa, Keijiro, Ram Kannan, and David R. Hinton. “Molecular mechanisms of subretinal fibrosis in age-related macular degeneration.” Experimental eye research 142 (2016): 19-25. ↩︎
Last Updated on by ayeshayusuf



